



















































Contraceptive Wants and Needs Among Women with Substance Use Disorders – R Street Institute
Advancing Sustainable Development Goals Through Improved Contraceptive Access for Women with Substance Use Disorder
A significant challenge to achieving Sustainable Development Goal 3 (Good Health and Well-being) and SDG 5 (Gender Equality) in the United States is the high rate of unintended pregnancies among women with Substance Use Disorder (SUD). While approximately one-third of all pregnancies are unintended, this figure escalates to between 80 and 90 percent for women with SUD. This disparity highlights a critical issue in public health that directly impacts maternal and infant well-being, reproductive autonomy, and progress toward the 2030 Agenda for Sustainable Development.
Health Disparities and the Impact on SDG 3 and SDG 5
The Intersection of Unintended Pregnancy and Substance Use Disorder
The convergence of untreated SUD and unintended pregnancy creates a compound risk profile that undermines key targets within SDG 3, particularly Target 3.1 (reduce maternal mortality) and Target 3.2 (end preventable deaths of newborns). The health consequences for this vulnerable population are severe and include:
- Increased risk of overdose for pregnant women.
- Higher incidence of low infant birth weight and preterm labor.
- Elevated risk of stillbirth.
- Associated risks of maternal depression and intimate partner violence.
Furthermore, the stigma associated with substance use during pregnancy often deters women from seeking essential prenatal healthcare and SUD treatment, exacerbating these negative outcomes and creating barriers to achieving universal health coverage as outlined in SDG 3.
Contraceptive Use Patterns and Barriers to Reproductive Autonomy
Research indicates that most women with SUD wish to avoid pregnancy, yet their access to and use of effective contraception are limited, directly contravening SDG Target 3.7 (ensure universal access to sexual and reproductive health-care services) and SDG Target 5.6 (ensure universal access to sexual and reproductive health and reproductive rights). Current usage patterns reveal significant disparities:
- Only about one-third of women with SUD regularly use contraception, compared to two-thirds of the general female population.
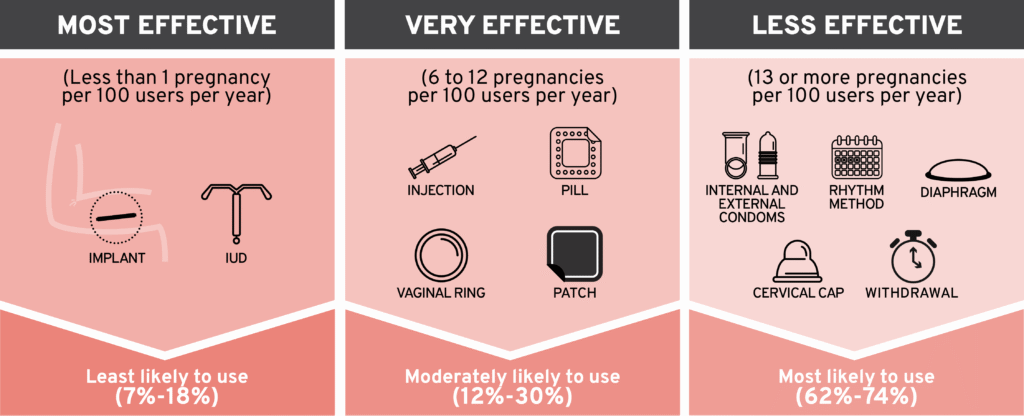
- Among those who use contraception, there is a high reliance on the least effective methods, such as condoms, withdrawal, and emergency contraception.
This gap between desire and practice points to systemic failures in providing equitable access to family planning, a cornerstone of both gender equality and public health.
Systemic Barriers to Achieving Health and Gender Equality (SDG 3, SDG 5, & SDG 10)
Addressing the low uptake of effective contraceptives requires an understanding of the multi-level barriers faced by women with SUD. These obstacles represent significant hurdles to reducing inequalities (SDG 10) and ensuring that no one is left behind.
Healthcare System Failures and Inequality
Structural and systemic barriers within the healthcare system are a primary cause of contraceptive access failure for this population. These barriers include:
- Stigma and Provider Attitudes: Fear of mistreatment and judgment from healthcare providers discourages engagement with the medical system.
- Logistical and Geographic Obstacles: Lack of transportation and significant distances to care facilities, particularly in areas known as “contraceptive deserts,” create physical barriers to access.
- Provider Shortages: A scarcity of qualified reproductive healthcare providers limits the availability of services.
- Financial Barriers: Insufficient insurance coverage and high out-of-pocket costs for both provider visits and contraceptive products are major deterrents. These financial obstacles directly challenge the goal of universal health access and perpetuate cycles of poverty (SDG 1).
Policy Recommendations for Accelerating Progress on the SDGs
A policy framework focused on lowering barriers and expanding choice is essential to empower women with SUD, improve health outcomes, and make tangible progress on the SDGs. The following policy solutions can effectively address cost and healthcare system inefficiencies.
-
Annual Supply Mandates
Permitting pharmacists to dispense a full 12-month supply of short-acting contraceptives (e.g., pill, patch, ring) in a single visit removes the barrier of frequent pharmacy or clinic visits. This policy directly supports SDG 3 by:
- Reducing unintended pregnancies and abortions.
- Increasing medication adherence and continuation rates.
- Generating significant cost savings for individuals, insurers, and governments.
-
Pharmacist Prescribing Authority
Expanding the scope of practice for pharmacists to include prescribing hormonal contraceptives leverages their accessibility to overcome geographic barriers. With over 95% of Americans living within 10 miles of a pharmacy, this policy helps reduce the inequalities (SDG 10) caused by “contraceptive deserts” and improves medication uptake, particularly for younger and uninsured women, thereby advancing SDG Target 3.7.
-
Over-the-Counter (OTC) Access
Making hormonal birth control available without a prescription provides the lowest-barrier access model. This is crucial for women who avoid clinical settings due to stigma. OTC access promotes reproductive autonomy (SDG 5) and has been shown to increase contraceptive uptake, especially among rural and uninsured women, directly contributing to the reduction of health inequalities (SDG 10).
Ensuring Affordability to Uphold Universal Access
The success of these policies is contingent upon affordability. To align with the principles of universal access central to the SDGs, public and private insurers must provide comprehensive coverage for a wide range of contraceptive products, including long-acting reversible contraception (LARC). Additionally, allowing Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs) to cover nonprescription medications can reduce the financial burden of OTC options.
Conclusion: A Call to Action for Sustainable Development
Women living with SUD desire and deserve control over their reproductive health. The high rate of unintended pregnancy in this population is not a personal failing but a systemic one, reflecting significant barriers to essential healthcare. By implementing policies that reduce costs and remove structural obstacles—such as annual supply, pharmacist prescribing, and OTC access—it is possible to make significant strides. These actions are not merely healthcare reforms; they are critical strategies for advancing SDG 3 (Good Health and Well-being), SDG 5 (Gender Equality), and SDG 10 (Reduced Inequalities), thereby supporting women’s autonomy and fostering a more equitable and sustainable society.
Analysis of Sustainable Development Goals in the Article
1. Which SDGs are addressed or connected to the issues highlighted in the article?
The article addresses issues that are directly connected to several Sustainable Development Goals (SDGs). The primary goals identified are:
- SDG 3: Good Health and Well-being: The core of the article revolves around public health issues, specifically focusing on the intersection of substance use disorder (SUD), unintended pregnancies, and maternal and infant health. It details the increased health risks for both mothers and infants, such as “overdose, low infant birth weight, preterm labor, stillbirth,” and discusses the importance of access to healthcare services, including prenatal care, SUD treatment, and contraception.
- SDG 5: Gender Equality: The article is centered on women’s health and empowerment. It highlights the desire of women with SUD to control their reproductive lives, stating that most “want to avoid pregnancy.” The discussion on facilitating access to contraceptives is framed as a way to increase women’s “autonomy and control over their reproductive health,” which is a fundamental aspect of gender equality.
- SDG 10: Reduced Inequalities: The article focuses on a specific, vulnerable population—women with a substance use disorder—who face disproportionately high rates of unintended pregnancy (“roughly 80 or 90 percent among women with a substance use disorder”) and greater barriers to healthcare compared to the general population. The proposed policy solutions aim to reduce these specific inequalities in health outcomes and access to care.
2. What specific targets under those SDGs can be identified based on the article’s content?
Based on the article’s discussion, several specific SDG targets can be identified:
- Under SDG 3 (Good Health and Well-being):
- Target 3.1: By 2030, reduce the global maternal mortality ratio. The article connects untreated SUD and unintended pregnancies to “a number of negative maternal and infant outcomes,” which implicitly includes the risk of maternal death. Improving contraceptive access is presented as a strategy to mitigate these risks.
- Target 3.2: By 2030, end preventable deaths of newborns and children under 5. The article explicitly mentions that untreated SUD increases the risk of “low infant birth weight, preterm labor, [and] stillbirth,” all of which contribute to infant mortality.
- Target 3.5: Strengthen the prevention and treatment of substance abuse. The entire context of the article is the health and well-being of women with substance use disorder (SUD). It highlights how stigma associated with SUD acts as a barrier to receiving both SUD treatment and prenatal healthcare.
- Target 3.7: By 2030, ensure universal access to sexual and reproductive health-care services, including for family planning. This is the central theme of the article. It details the low contraceptive use among women with SUD and advocates for policies like “Annual Supply,” “Pharmacist Prescribing,” and “Over the Counter” options to eliminate barriers and improve access to family planning.
- Under SDG 5 (Gender Equality):
- Target 5.6: Ensure universal access to sexual and reproductive health and reproductive rights. The article advocates for policies that give women with SUD “autonomy and control over their reproductive health and recovery journeys.” This aligns directly with ensuring reproductive rights and access to the necessary services to exercise those rights.
- Under SDG 10 (Reduced Inequalities):
- Target 10.3: Ensure equal opportunity and reduce inequalities of outcome. The article highlights a significant inequality of outcome: women with SUD have much higher rates of unintended pregnancy and lower rates of contraceptive use than the general population. The proposed policies are designed to reduce this specific health inequality by removing systemic barriers to care.
3. Are there any indicators mentioned or implied in the article that can be used to measure progress towards the identified targets?
Yes, the article mentions or implies several quantitative and qualitative indicators that can be used to measure progress:
- Rate of Unintended Pregnancy: The article provides a baseline indicator by stating that “about one-third of pregnancies in the United States are unintended, and that proportion almost triples to roughly 80 or 90 percent among women with a substance use disorder.” A reduction in this rate for women with SUD would indicate progress.
- Contraceptive Use Rate: The article provides a clear indicator by comparing contraceptive use: “only about one-third [of women with SUD] regularly use contraception compared to two-thirds of American women generally.” Progress could be measured by the increase in regular contraceptive use among women with SUD.
- Uptake of Effective Contraceptive Methods: An indicator is implied in the statement that women with SUD who use contraception are “most likely to use the least reliable methods.” An increase in the use of more effective methods like hormone pills and LARC would signify progress.
- Maternal and Infant Health Outcomes: The article lists specific negative outcomes like “low infant birth weight, preterm labor, [and] stillbirth.” The incidence rates of these outcomes among women with SUD can serve as direct indicators of health and well-being.
- Access to Healthcare Providers: The article mentions that “between 17 percent and 50 percent of American women lived in a ‘contraceptive desert’ in 2018.” A reduction in this percentage, particularly for vulnerable populations, would be a key indicator of improved access.
- Healthcare Costs: The article suggests an economic indicator by noting that reducing unintended pregnancies “saves money for insurers and governments.” Tracking these cost savings could measure the financial efficiency and benefit of the proposed policies.
4. Table of SDGs, Targets, and Indicators
| SDGs | Targets | Indicators Identified in the Article |
|---|---|---|
| SDG 3: Good Health and Well-being |
3.1: Reduce maternal mortality. 3.2: End preventable deaths of newborns. 3.5: Strengthen prevention and treatment of substance abuse. 3.7: Ensure universal access to sexual and reproductive health-care services. |
– Incidence of negative maternal outcomes (e.g., overdose). – Rates of low infant birth weight, preterm labor, and stillbirth. – Proportion of women with SUD engaged in treatment and prenatal care. – Rate of unintended pregnancies among women with SUD (currently 80-90%). – Proportion of women with SUD regularly using contraception (currently ~33%). |
| SDG 5: Gender Equality | 5.6: Ensure universal access to sexual and reproductive health and reproductive rights. |
– Rate of uptake of various contraceptive methods, reflecting choice and autonomy. – Proportion of women with SUD using effective contraceptive methods (vs. “least reliable methods”). – Qualitative measures of women’s reported autonomy over their reproductive health. |
| SDG 10: Reduced Inequalities | 10.3: Ensure equal opportunity and reduce inequalities of outcome. |
– The gap in contraceptive use rates between women with SUD (~33%) and the general female population (~66%). – The gap in unintended pregnancy rates between women with SUD (80-90%) and the general population (~33%). – Percentage of women living in a “contraceptive desert” (currently 17-50%). |
Source: rstreet.org
What is Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0