




















































The quiet collapse of America’s reproductive health safety net – CBS News
Report on the Impact of U.S. Reproductive Healthcare Funding Cuts on Sustainable Development Goals
Introduction and Summary
Recent federal funding cuts and the administrative shutdown of the Title X Family Planning Program in the United States represent a significant setback for multiple Sustainable Development Goals (SDGs). The closure of reproductive health clinics, such as those operated by Maine Family Planning, directly impacts the nation’s progress towards ensuring good health, achieving gender equality, reducing poverty, and promoting strong institutions. This report analyzes the consequences of these policy changes on the advancement of the SDGs.
Erosion of Progress Towards SDG 3: Good Health and Well-being
The termination of funding and operational support for family planning services directly contravenes the objectives of SDG 3, which aims to ensure healthy lives and promote well-being for all at all ages.
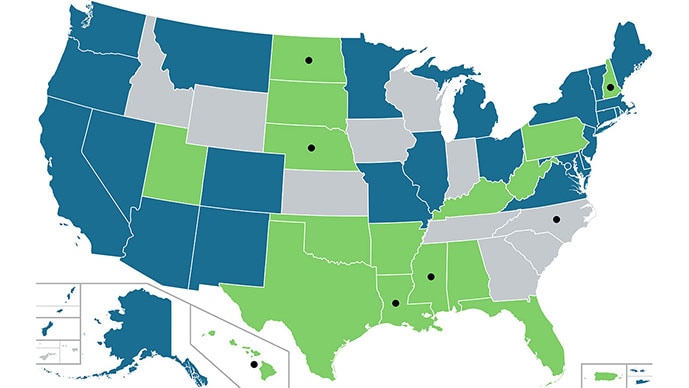
- Undermining Universal Access (Target 3.7): The closure of clinics that provide contraception, STI testing, cancer screenings, and primary care removes essential health services for low-income, uninsured, and rural populations. The shutdown of the Office of Population Affairs (OPA) jeopardizes a network of over 4,000 clinics serving nearly 3 million patients annually.
- Increased Maternal and Infant Health Risks: Family planning is a critical component of maternal health, allowing for the management of chronic conditions like hypertension and diabetes before pregnancy. The lack of access to these services is projected to lead to a rise in unplanned pregnancies, which carry higher health risks and contribute to increased maternal mortality, particularly among vulnerable communities.
- Disruption of Preventive Care (Target 3.8): Title X clinics are often the sole providers of preventive care, including cancer screenings and STI testing, for uninsured individuals. The erosion of this healthcare safety net, compounded by cuts to Medicaid and the CDC, increases the likelihood of later-stage disease diagnoses and poorer health outcomes.
Setbacks for SDG 5 (Gender Equality) and SDG 1 (No Poverty)
Access to reproductive healthcare is intrinsically linked to gender equality, economic empowerment, and poverty reduction. The current situation undermines progress on both SDG 5 and SDG 1.
- Diminished Autonomy and Opportunity (SDG 5): The ability to plan and space pregnancies is fundamental to women’s health, autonomy, and their ability to pursue educational and economic opportunities. Restricting access to family planning disproportionately impacts women, hindering their empowerment and reinforcing gender inequality.
- Economic Disempowerment (SDG 1): Historical data demonstrates a direct link between access to family planning and economic well-being. Research indicates that children born after the establishment of federally-funded family planning programs were 7% less likely to live in poverty. Furthermore, providing free birth control to low-income women has been shown to reduce unintended pregnancies and abortions, contributing to greater household financial stability.
- Fiscal Inefficiency: The cuts are counterproductive from a fiscal standpoint. Analysis shows that every dollar invested in publicly funded family planning saves approximately seven dollars in Medicaid costs related to pregnancy and childbirth. The current policy is projected to increase long-term public expenditure.
Exacerbating Inequalities in Contravention of SDG 10
The impact of the clinic closures and funding freezes is not evenly distributed, thereby worsening existing disparities and working against the aims of SDG 10 (Reduced Inequalities).
- Disproportionate Impact on Vulnerable Populations: The communities most affected are rural, low-income, uninsured, Black, and Indigenous populations, who already face significant barriers to healthcare.
- Expansion of “Contraceptive Deserts”: Over 19 million women in the U.S. already reside in areas with limited access to publicly supported contraceptive services. The current crisis will expand these “deserts,” forcing individuals to travel prohibitive distances for essential care.
- Widening Gaps in Health Outcomes: The predictable consequences include higher rates of untreated infections, unintended pregnancies, and maternal deaths, further widening the health equity gap between privileged and marginalized communities.
Weakening of Public Institutions (SDG 16)
The “functional elimination” of the OPA through staff reductions and operational halts represents a weakening of effective and accountable public institutions, a key target of SDG 16.
- Dismantling of Health Infrastructure: The OPA, which has managed the nation’s family planning program for over 50 years, has been reduced from a staff of approximately 40-50 individuals to a single officer. This dismantles the administrative structure required to run a national public health program.
- Suspension of Governance and Oversight: With the OPA offline, no new funds can be distributed, and critical functions such as compliance reviews, clinical guidance, and technical assistance are suspended. This creates a vacuum in oversight and quality control.
- Threat of Systemic Collapse: Without federal administration and funding, the entire network of Title X clinics is at risk of collapse. While some states are attempting to fill the gap, these efforts are insufficient to replace federal support at scale, threatening a foundational component of the U.S. public health system.
Analysis of the Article in Relation to Sustainable Development Goals
-
Which SDGs are addressed or connected to the issues highlighted in the article?
The article primarily addresses issues related to several Sustainable Development Goals (SDGs) by highlighting the consequences of funding cuts to reproductive and primary healthcare services in the United States.
- SDG 3: Good Health and Well-being: This is the most central SDG discussed. The article focuses on the closure of health clinics, loss of access to primary and preventive care, reproductive health services, and the resulting negative health outcomes, such as increased maternal mortality and untreated infections.
- SDG 5: Gender Equality: The article directly connects access to family planning with women’s health, autonomy, and economic opportunity. It emphasizes that the “ability to time and space pregnancies was absolutely essential to women’s and children’s health,” framing reproductive care as a cornerstone of female empowerment.
- SDG 1: No Poverty: The article establishes a clear link between family planning and poverty reduction. It cites research showing that children born after the implementation of federally-funded family-planning programs were “7% less likely to live in poverty” and had higher household incomes.
- SDG 10: Reduced Inequalities: The issues disproportionately affect vulnerable and marginalized populations. The article specifies that the people “hit hardest are rural, low-income, and uninsured” and predicts “more maternal deaths, especially among Black, Indigenous, and rural communities,” highlighting the widening health inequalities.
-
What specific targets under those SDGs can be identified based on the article’s content?
Several specific SDG targets are relevant to the challenges described in the article.
- Target 3.1: By 2030, reduce the global maternal mortality ratio. The article warns that if clinics close, “we’ll see… more maternal deaths.” It explains that family planning is crucial for maternal health as it allows women to manage conditions like “high blood pressure, diabetes, and heart disease before pregnancy.”
- Target 3.7: By 2030, ensure universal access to sexual and reproductive health-care services, including for family planning, information and education. The entire article is about the dismantling of this access. The shutdown of the Title X program, which served “nearly 3 million low-income or uninsured patients annually” with services like “contraception, pregnancy testing, testing and treatment for sexually transmitted infections,” is a direct setback to this target.
- Target 3.8: Achieve universal health coverage, including financial risk protection, access to quality essential health-care services. The article details how the closure of clinics that served “uninsured or on Medicaid” patients erodes the healthcare safety net, leaving vulnerable populations without access to “primary and preventive care.”
- Target 5.6: Ensure universal access to sexual and reproductive health and reproductive rights. The article frames family planning as a fundamental component of health and autonomy. The creation of “contraceptive deserts,” where “more than 19 million women” lack reasonable access to birth control, directly undermines this target.
- Target 1.3: Implement nationally appropriate social protection systems and measures for all… and achieve substantial coverage of the poor and the vulnerable. The article describes Title X, Medicaid, and ACA subsidies as a “broader safety net.” The funding cuts and program shutdowns represent a failure to maintain these social protection systems for the “low-income or uninsured patients” who rely on them.
- Target 10.2: By 2030, empower and promote the social, economic and political inclusion of all, irrespective of age, sex, disability, race, ethnicity, origin, religion or economic or other status. The article shows how the loss of healthcare access leads to the exclusion of people based on their economic status (“low-income,” “uninsured”) and geographic location (“rural communities”), hindering their ability to maintain their health and economic stability.
-
Are there any indicators mentioned or implied in the article that can be used to measure progress towards the identified targets?
The article mentions or implies several quantitative and qualitative indicators that can be used to measure progress.
- Indicator for Target 3.7 (Access to Family Planning): The article provides a direct indicator of need by stating that “more than 19 million women” live in “contraceptive deserts.” A reduction in this number would indicate progress. Furthermore, the article mentions that when low-income women access free birth control, “unintended pregnancies drop by 16%,” providing a clear metric for success.
- Indicator for Target 3.8 (Health Service Coverage): The number of clinics and patients served is a key indicator. The article mentions the national network of “over 4,000 clinics” under Title X serving “nearly 3 million low-income or uninsured patients annually.” The closure of these clinics, such as the “three rural clinics in northern Maine” serving “800 patients,” is a direct negative indicator of health service coverage.
- Indicator for Target 3.1 (Maternal Health): While not providing a current rate, the article implies that the maternal mortality rate is a key indicator, warning of “more maternal deaths” as a consequence of the cuts. The prevalence of pre-existing conditions like “peripartum cardiomyopathy” that are dangerous during pregnancy also serves as an indirect indicator of the need for pre-conception care.
- Indicator for Target 1.3 (Social Protection Systems): The article points to the economic efficiency of these programs as an indicator. It states that “every $1 invested in publicly funded family-planning programs saves roughly $7 in Medicaid costs.” This cost-benefit ratio serves as a powerful indicator of the program’s value as a social protection measure.
- Indicator for Target 10.2 (Inequality): The article implies the use of disaggregated data to measure inequality. It specifically calls out the disproportionate impact on “Black, Indigenous, and rural communities.” Therefore, indicators such as rates of unintended pregnancy, STI infection, and maternal mortality, when broken down by race and location, would measure progress toward reducing these inequalities.
Summary of SDGs, Targets, and Indicators
| SDGs | Targets | Indicators Identified in the Article |
|---|---|---|
| SDG 3: Good Health and Well-being |
3.1: Reduce maternal mortality.
3.7: Ensure universal access to sexual and reproductive health-care services. 3.8: Achieve universal health coverage. |
– Predicted increase in “maternal deaths.” – Number of women living in “contraceptive deserts” (19 million). – Percentage drop in unintended pregnancies with access to birth control (16%). – Number of clinics providing services (network of 4,000) and number of patients served (nearly 3 million annually). |
| SDG 5: Gender Equality | 5.6: Ensure universal access to sexual and reproductive health and reproductive rights. |
– Access to family planning as essential for women’s “health and autonomy.” – Lack of “reasonable access to publicly supported birth control” for millions of women. |
| SDG 1: No Poverty | 1.3: Implement social protection systems for the poor and vulnerable. |
– Percentage of children less likely to live in poverty due to family planning programs (7%). – Return on investment for public spending on family planning ($7 saved for every $1 invested). |
| SDG 10: Reduced Inequalities | 10.2: Empower and promote the inclusion of all, irrespective of economic or other status. |
– Disproportionate negative health impacts on “Black, Indigenous, and rural communities.” – Specific focus on services for “low-income,” “uninsured,” and “Medicaid” patients who are losing access. |
Source: cbsnews.com
What is Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0