




























































The association between air pollution and cardiovascular health in middle-aged and older Chinese adults: cross-sectional and prospective analyses – Nature
Executive Summary
A study utilizing data from the China Health and Retirement Longitudinal Study (CHARLS) investigated the association between long-term exposure to ambient air pollutants and heart disease risk among middle-aged and older adults in China. This research directly addresses several Sustainable Development Goals (SDGs), particularly SDG 3 (Good Health and Well-being) by examining non-communicable diseases, SDG 10 (Reduced Inequalities) by identifying vulnerable populations, and SDG 11 (Sustainable Cities and Communities) by highlighting the health impacts of urban and rural air quality. A prospective analysis following 7,750 participants over nine years found that long-term exposure to particulate matter (PM₁, PM₂.₅, and PM₁₀) was robustly associated with an increased risk of incident heart disease. These findings underscore air pollution as a critical modifiable risk factor, emphasizing the need for targeted public health strategies to protect susceptible groups—including women, rural residents, and individuals with lower education—and advance the 2030 Agenda for Sustainable Development.
Introduction: Air Pollution, Public Health, and Sustainable Development
The Global Burden of Cardiovascular Disease and SDG 3
Cardiovascular disease (CVD) represents a primary obstacle to achieving SDG 3 (Good Health and Well-being), particularly Target 3.4, which aims to reduce premature mortality from non-communicable diseases (NCDs). As the leading cause of death globally and in China, CVD, and specifically heart disease, imposes a significant burden on public health systems and undermines sustainable development. Addressing the environmental determinants of NCDs is crucial for making progress on this global goal.
Air Pollution as a Barrier to Sustainable Health Outcomes
Air pollution is a major environmental threat that directly contravenes the objectives of multiple SDGs. Its role as a modifiable risk factor for CVD is well-established, linking directly to public health priorities under SDG 3. Furthermore, managing air quality is a core component of SDG 11 (Sustainable Cities and Communities), which calls for reducing the adverse per capita environmental impact of cities (Target 11.6). This study investigates the long-term health consequences of exposure to multiple pollutants (PM₁, PM₂.₅, PM₁₀, NO₂, and O₃) to provide evidence for policies that can simultaneously improve public health and promote environmental sustainability.
Methodology: A National Cohort Study in China
Study Population and Design
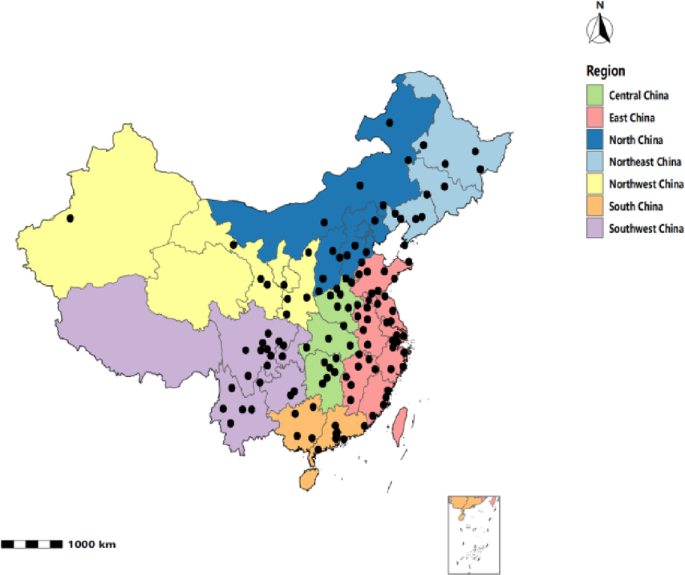
The study utilized nationally representative data from the China Health and Retirement Longitudinal Study (CHARLS), a multistage survey of Chinese adults aged 45 and older.
- Cross-sectional analysis: Included 9,403 participants from the 2011 baseline.
- Prospective analysis: Followed a cohort of 7,750 participants free of heart disease at baseline for nine years (2011–2020).
Air Pollution Exposure Assessment
Annual average concentrations of five key air pollutants were estimated using the high-resolution spatiotemporal China High Air Pollution (CHAP) model. Exposures were assigned to participants based on city-level geocoded residential information, providing a basis for assessing the environmental health risks relevant to SDG 11.
Outcome and Covariate Assessment
The primary health outcome was incident heart disease, identified through self-reported physician diagnoses. A comprehensive set of covariates was included to control for potential confounding factors:
- Sociodemographic Characteristics: Age, sex, marital status, educational level, and place of residence (urban/rural).
- Lifestyle Factors: Sleep duration, smoking status, and alcohol consumption.
- Clinical Conditions: Body Mass Index (BMI), hypertension, and diabetes.
Statistical Analysis
Logistic regression models were used for cross-sectional analysis, while Cox proportional hazards models were applied to the longitudinal data to estimate the risk of incident heart disease. The analysis included single-pollutant models, multi-pollutant models, and extensive sensitivity tests to ensure the robustness of the findings.
Results: Quantifying the Health Impacts of Air Pollution
Longitudinal Analysis of Incident Heart Disease
The prospective analysis revealed a significant and robust association between long-term exposure to particulate matter and an increased risk of heart disease, a critical finding for advancing SDG 3.
- A 1-standard deviation (SD) increase in PM₁₀ was associated with a 22.3% higher risk of incident heart disease.
- A 1-SD increase in PM₂.₅ was associated with a 15.1% higher risk.
- PM₁ and NO₂ were also positively associated with incident risk.
- The association for O₃ was not significant in single-pollutant models and showed instability in multi-pollutant models.
Multi-Pollutant Model Findings
In models adjusting for co-pollutants, the associations for PM₂.₅ and PM₁₀ remained consistently positive and statistically significant. This suggests that the adverse cardiovascular effects of particulate matter are independent of other gaseous pollutants, reinforcing the need for targeted PM reduction strategies to meet public health and sustainability targets.
Identifying Vulnerable Populations: Aligning with SDG 10
Subgroup analyses were conducted to explore population heterogeneity, providing insights relevant to SDG 10 (Reduced Inequalities) and SDG 5 (Gender Equality). Although interaction tests were not statistically significant, stratified results suggested higher risk estimates for specific demographic groups:
- Women
- Rural residents
- Individuals with lower educational attainment
These trends indicate that the health burden of air pollution may be disproportionately borne by socially and economically disadvantaged groups, highlighting the need for equitable environmental health policies.
Discussion: Implications for Public Health Policy and SDGs
Particulate Matter as a Primary Health Threat
The study confirms that long-term exposure to particulate matter (PM₁, PM₂.₅, and PM₁₀) is a significant risk factor for heart disease in China’s aging population. This evidence provides a strong rationale for implementing stricter air quality standards and pollution control measures, which are essential for achieving the health-related targets of SDG 3 and creating healthier living environments as envisioned in SDG 11.
Addressing Inequalities and Protecting Vulnerable Groups (SDG 5, SDG 10)
The findings that women, rural residents, and those with lower education may face elevated risks underscore the importance of an equity-focused approach to public health. To align with the “leave no one behind” principle of the 2030 Agenda, policies must address the specific vulnerabilities of these populations. This involves not only broad environmental regulations but also targeted interventions, health education, and improved healthcare access for at-risk communities, thereby contributing to SDG 10 and SDG 5.
Study Strengths and Limitations
The study’s strengths include its use of a nationally representative cohort, a longitudinal design, and a comprehensive analysis of multiple pollutants. However, limitations include the use of city-level exposure data, which may not capture individual-level variability, and self-reported health outcomes. Despite these limitations, the study provides valuable evidence on the public health consequences of air pollution in China.
Conclusion: Advancing Health and Sustainability through Air Quality Management
This study demonstrates that long-term exposure to particulate matter is significantly associated with an increased risk of heart disease among middle-aged and older adults in China. The findings highlight that particulate matter pollution is a critical modifiable risk factor, and its reduction is paramount for public health. By framing these results within the context of the Sustainable Development Goals, it becomes clear that improving air quality is not only an environmental issue but a fundamental requirement for achieving good health and well-being (SDG 3), reducing inequalities (SDG 10), and building sustainable communities (SDG 11). Targeted public health strategies are urgently needed to protect vulnerable populations and mitigate the substantial burden of cardiovascular disease attributable to air pollution.
Analysis of Sustainable Development Goals (SDGs) in the Article
1. Which SDGs are addressed or connected to the issues highlighted in the article?
-
SDG 3: Good Health and Well-being
The article is fundamentally a public health study that directly addresses SDG 3. It investigates the health impacts of environmental factors on human populations.
- Connection to the Article: The study’s primary focus is on the association between ambient air pollution and the risk of heart disease, a leading non-communicable disease (NCD). The introduction states that “Cardiovascular disease (CVD) is among the most prevalent non-communicable diseases (NCDs) worldwide, accounting for nearly one-third of all global deaths.” This directly aligns with the goal of promoting well-being and addressing major health threats.
-
SDG 11: Sustainable Cities and Communities
The research context is centered on air quality, a critical component of urban environmental health and sustainability.
- Connection to the Article: The study analyzes the impact of “ambient air pollutants” such as PM₂,₅, PM₁₀, and NO₂, which are major problems in urban and industrial areas. The data on pollution was “assigned to participants based on city-level geocoded residential information,” explicitly linking the environmental hazard to urban and semi-urban settings. The article notes that China faces “persistently high pollution levels driven by rapid urbanization and industrialization,” reinforcing the connection to sustainable urban development.
-
SDG 10: Reduced Inequalities
The article identifies specific demographic groups that are disproportionately affected by air pollution, highlighting inequalities in health outcomes.
- Connection to the Article: The subgroup analysis found that the health risks associated with air pollution were not evenly distributed. The article states that “stratified analyses suggested that women, individuals with lower educational attainment, and rural residents had higher risk estimates associated with exposure to PM₁, PM₂.₅, and PM₁₀.” This finding directly relates to the goal of reducing inequalities by showing how environmental burdens disproportionately harm vulnerable populations.
2. What specific targets under those SDGs can be identified based on the article’s content?
-
Targets under SDG 3 (Good Health and Well-being)
- Target 3.4: By 2030, reduce by one-third premature mortality from non-communicable diseases through prevention and treatment and promote mental health and well-being.
Explanation: The article focuses on heart disease, a primary NCD. By identifying air pollution as a “modifiable risk factor,” the study provides evidence that is crucial for developing “prevention” strategies to reduce premature mortality from cardiovascular diseases. The conclusion emphasizes the need for “targeted public health strategies to protect vulnerable populations and reduce the burden of HD.” - Target 3.9: By 2030, substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water and soil pollution and contamination.
Explanation: This target is directly addressed. The entire study is designed to quantify the “increased risk of heart disease” (illness) associated with long-term exposure to specific air pollutants (PM₁, PM₂.₅, PM₁₀, NO₂). The introduction cites a Global Burden of Disease study, noting that “in 2015, air pollution–related diseases accounted for approximately 4.2 million deaths worldwide,” directly linking air pollution to deaths and illnesses.
- Target 3.4: By 2030, reduce by one-third premature mortality from non-communicable diseases through prevention and treatment and promote mental health and well-being.
-
Target under SDG 11 (Sustainable Cities and Communities)
- Target 11.6: By 2030, reduce the adverse per capita environmental impact of cities, including by paying special attention to air quality and municipal and other waste management.
Explanation: The study’s methodology relies on measuring urban air quality. It uses “annual average concentrations of PM₁, PM₂.₅, PM₁₀, NO₂, and O₃” assigned at the city level to assess the environmental impact on residents. The findings, which show a robust link between particulate matter pollution and heart disease, underscore the urgency of improving urban air quality to reduce its adverse health effects, directly aligning with this target.
- Target 11.6: By 2030, reduce the adverse per capita environmental impact of cities, including by paying special attention to air quality and municipal and other waste management.
-
Target under SDG 10 (Reduced Inequalities)
- Target 10.2: By 2030, empower and promote the social, economic and political inclusion of all, irrespective of age, sex, disability, race, colour, ethnicity, origin, religion or economic or other status.
Explanation: While the article does not discuss social or political inclusion, its findings provide the evidence base needed to address health inequalities. By identifying that “women, individuals with lower education, and rural residents” face a higher risk, the study highlights a disparity in health outcomes based on sex, socioeconomic status (proxied by education), and geographic location. Addressing these disparities is a core component of achieving the inclusive aim of Target 10.2.
- Target 10.2: By 2030, empower and promote the social, economic and political inclusion of all, irrespective of age, sex, disability, race, colour, ethnicity, origin, religion or economic or other status.
3. Are there any indicators mentioned or implied in the article that can be used to measure progress towards the identified targets?
-
Indicators for SDG 3 Targets
- Indicator 3.4.1: Mortality rate attributed to cardiovascular disease, cancer, diabetes or chronic respiratory disease.
Implied in the Article: The study’s outcome is “incident heart disease,” a major cardiovascular disease. The introduction explicitly mentions that CVD was “responsible for approximately 5.09 million deaths in China” and that “cardiovascular mortality” accounts for a significant portion of pollution-related deaths. The hazard ratios (e.g., “HR = 1.223” for PM₁₀) are statistical measures of risk that directly contribute to understanding and calculating the mortality rate attributable to CVD from specific risk factors. - Indicator 3.9.1: Mortality rate attributed to household and ambient air pollution.
Mentioned in the Article: The article directly references data for this indicator by citing the Global Burden of Disease study, which “reported that, in 2015, air pollution–related diseases accounted for approximately 4.2 million deaths worldwide, representing 7.6% of all global deaths.” The study’s entire purpose is to strengthen the evidence linking ambient air pollution to adverse health outcomes that contribute to this mortality rate.
- Indicator 3.4.1: Mortality rate attributed to cardiovascular disease, cancer, diabetes or chronic respiratory disease.
-
Indicator for SDG 11 Target
- Indicator 11.6.2: Annual mean levels of fine particulate matter (e.g. PM2.5 and PM10) in cities (population weighted).
Mentioned in the Article: The study explicitly uses this indicator as its primary exposure variable. The methods section states, “Annual average concentrations of PM₁, PM₂.₅, PM₁₀, NO₂, and O₃ were estimated… and assigned to participants based on city-level geocoded residential information.” The concentrations are measured in micrograms per cubic meter (µg/m³), which is the standard unit for this official SDG indicator.
- Indicator 11.6.2: Annual mean levels of fine particulate matter (e.g. PM2.5 and PM10) in cities (population weighted).
-
Indicator for SDG 10 Target
- Disaggregated Health Data: While not a formal SDG indicator, the principle of disaggregation is key to monitoring SDG 10. Progress towards Target 10.2 is measured by analyzing outcomes across different demographic groups.
Implied in the Article: The study provides data disaggregated by demographic characteristics. The “Subgroup and interaction analyses” section examines health risks stratified by “sex, age… residence (urban/rural), education, smoking, drinking, diabetes, and hypertension.” Finding higher risks for women, rural residents, and those with lower education provides a direct measure of inequality in health outcomes related to environmental exposure.
- Disaggregated Health Data: While not a formal SDG indicator, the principle of disaggregation is key to monitoring SDG 10. Progress towards Target 10.2 is measured by analyzing outcomes across different demographic groups.
4. Table of SDGs, Targets, and Indicators
| SDGs | Targets | Indicators Identified in the Article |
|---|---|---|
| SDG 3: Good Health and Well-being | 3.4: Reduce premature mortality from non-communicable diseases (NCDs).
3.9: Substantially reduce deaths and illnesses from air pollution. |
For 3.4: Incidence and prevalence of heart disease (a major NCD); Hazard Ratios (HR) linking pollution to increased risk of cardiac events. (Proxy for Indicator 3.4.1: Mortality rate attributed to cardiovascular disease).
For 3.9: Number of deaths attributed to air pollution-related diseases (e.g., “4.2 million deaths worldwide”); Risk of heart disease associated with exposure to specific pollutants. (Directly relates to Indicator 3.9.1: Mortality rate attributed to ambient air pollution). |
| SDG 11: Sustainable Cities and Communities | 11.6: Reduce the adverse per capita environmental impact of cities, paying special attention to air quality. | For 11.6: “Annual average concentrations of PM₁, PM₂.₅, PM₁₀, NO₂, and O₃” measured in µg/m³ at the city level. (Directly corresponds to Indicator 11.6.2: Annual mean levels of fine particulate matter in cities). |
| SDG 10: Reduced Inequalities | 10.2: Empower and promote the inclusion of all, irrespective of sex, age, economic or other status. | For 10.2: Disaggregated health risk data showing higher risk of heart disease from pollution among specific subgroups: “women, individuals with lower educational attainment, and rural residents.” (Proxy indicator measuring inequality in health outcomes). |
Source: nature.com
What is Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0











