






























































WHO Warns of Worsening Global Cholera Crisis as U.S. Aid Declines – Global Biodefense

Global Cholera Resurgence: A Threat to Sustainable Development Goals
Cholera Outbreak Analysis and Impact on SDG 3
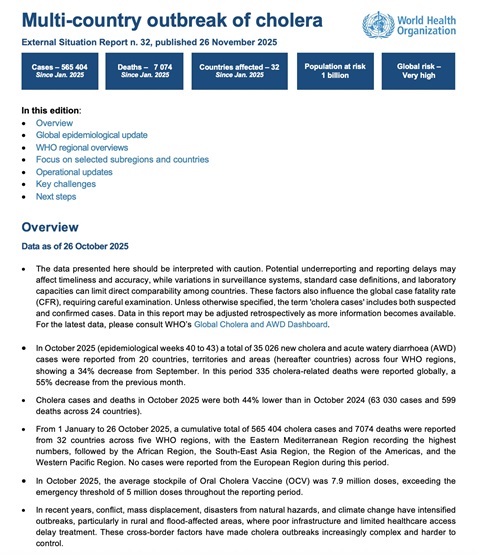
A significant global resurgence of cholera is actively undermining progress toward Sustainable Development Goal 3 (Good Health and Well-being). According to a World Health Organization report, the period from January to August 2025 saw a severe escalation of the crisis, directly threatening Target 3.3, which aims to end epidemics of communicable diseases. The data indicates a failure in global public health systems to manage preventable diseases.
- Total Cases Reported: 462,890
- Total Deaths Reported: 5,869
- Countries Affected: 32
- Increase in Fatalities: 118% compared to the same period in 2024
The WHO has classified the global risk level as “very high,” noting that conflict and climate shocks exacerbate the situation, particularly in the African and Eastern Mediterranean Regions. This crisis highlights systemic weaknesses in healthcare access, which is a core component of SDG 3.
The Central Role of SDG 6 in Cholera Transmission
Scientific modeling reinforces the direct link between the cholera epidemic and a lack of progress on SDG 6 (Clean Water and Sanitation). A study in BMC Public Health identified inadequate sanitation and contaminated water as primary drivers of transmission. The research established a median basic reproduction number (R₀) of 2.0, indicating that the absence of clean water and sanitation infrastructure allows the disease to spread exponentially. This situation is compounded by extreme weather events, linking the crisis to SDG 13 (Climate Action), as climate shocks damage already fragile water systems.
Proactive Interventions: A Model for Achieving the SDGs
A successful pilot program in the Democratic Republic of the Congo (DRC) demonstrates an effective model for achieving the SDGs through multi-stakeholder collaboration. This initiative exemplifies SDG 17 (Partnerships for the Goals), uniting OCHA, WHO, UNICEF, and the DRC’s national cholera program.
- An anticipatory action framework linked real-time surveillance data to pre-authorized humanitarian financing.
- When outbreak thresholds were met, the UN Central Emergency Response Fund (CERF) rapidly released $750,000.
- The funds enabled the provision of chlorinated water, sanitation facilities, and new treatment centers to over 230,000 people.
The result was a case fatality rate of only 0.27%, significantly below the 1% global benchmark. This proves that proactive, data-driven partnerships can accelerate progress toward SDG 3 by saving lives and building resilient health responses.
Funding Deficits and the Undermining of SDG 6 and SDG 17
Despite proven solutions, a decline in international aid commitments threatens to reverse progress. An analysis by the Center for Global Development (CGD) revealed that a 2025 U.S. aid freeze, which suspended funding for Water, Sanitation, and Hygiene (WASH) programs, correlated with a surge in cholera mortality in Africa. This directly undermines SDG 6 by defunding the essential infrastructure needed to prevent waterborne diseases. The reduction in aid represents a setback for SDG 17, as it weakens the international cooperation required to address global health challenges and support the most vulnerable nations.
Cholera as a Global Security Threat to SDG 16
The resurgence of cholera is not only a humanitarian crisis but also a threat to global health security and, by extension, SDG 16 (Peace, Justice and Strong Institutions). The conditions that fuel cholera—fragile infrastructure, population displacement, and weak governance—also create instability and are conducive to other disease outbreaks. Investing in the public health systems needed to control cholera is a strategic imperative for building peaceful and resilient societies, as disease outbreaks can destabilize regions and have cross-border implications.
Strategic Recommendations for Advancing the 2030 Agenda
Evidence from global health bodies and scientific research points to clear priorities for aligning the cholera response with the Sustainable Development Goals.
- Expand Anticipatory Financing: Implement and scale locally triggered financing mechanisms to ensure rapid response before outbreaks escalate, directly supporting SDG 3 and SDG 17.
- Sustain International Aid for WASH: Rebuild and protect international aid commitments for water, sanitation, and hygiene infrastructure as a foundational requirement for achieving SDG 6.
- Integrate Data and Modeling: Utilize mathematical modeling and real-time data in national control programs to improve prediction and containment, advancing SDG 3 through innovation aligned with SDG 9 (Industry, Innovation and Infrastructure).
- Strengthen Public Health as a Pillar of Security: Recognize that investment in public health infrastructure is essential for national and global stability, contributing to the objectives of SDG 3 and SDG 16.
Analysis of Sustainable Development Goals in the Article
-
Which SDGs are addressed or connected to the issues highlighted in the article?
The article on the resurgence of cholera directly addresses and connects to several Sustainable Development Goals (SDGs), primarily focusing on health, water and sanitation, and global partnerships.
- SDG 3: Good Health and Well-being: This is the most central SDG, as the entire article revolves around cholera, a preventable communicable disease. It discusses the scale of the epidemic (462,890 cases and 5,869 deaths), the strain on healthcare systems, mortality rates, and public health interventions. The article frames cholera not just as a humanitarian issue but as a “health-security concern.”
- SDG 6: Clean Water and Sanitation: The article explicitly states that cholera “thrives where clean water and sanitation are scarce.” It identifies “waterborne transmission” and “inadequate sanitation” as key drivers of the epidemic. Furthermore, it highlights the critical role of Water, Sanitation, and Hygiene (WASH) initiatives in both prevention and response, noting that a U.S. aid freeze excluded preventive measures like WASH, which correlated with a surge in cholera mortality.
- SDG 1: No Poverty: The article connects the cholera crisis to underlying vulnerabilities often associated with poverty. It mentions that “limited healthcare access, climate shocks, and conflict-driven displacement” amplify the disease’s reach. These factors disproportionately affect poor and vulnerable populations, highlighting the link between poverty, resilience, and health outcomes.
- SDG 17: Partnerships for the Goals: The article underscores the importance of global cooperation and financing. It details a successful partnership in the Democratic Republic of the Congo involving OCHA, WHO, UNICEF, and the national government. Conversely, it critiques the failure of partnerships, citing the “U.S. funding freeze” and its detrimental impact on cholera control, emphasizing the need to “rebuild and sustain international aid commitments.”
-
What specific targets under those SDGs can be identified based on the article’s content?
The article’s content points to several specific targets within the identified SDGs.
-
Under SDG 3 (Good Health and Well-being):
- Target 3.3: “By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.” The article is entirely focused on combating cholera, a major water-borne disease, and discusses the failure to contain its spread, as evidenced by the rising number of cases and deaths.
- Target 3.d: “Strengthen the capacity of all countries, in particular developing countries, for early warning, risk reduction and management of national and global health risks.” The article highlights the success of the “anticipatory action framework” in the DRC, which used real-time surveillance and pre-authorized financing as an early warning and response system. It also calls for integrating modeling and real-time data into national control programs to manage health risks better.
-
Under SDG 6 (Clean Water and Sanitation):
- Target 6.1: “By 2030, achieve universal and equitable access to safe and affordable drinking water for all.” The article identifies the lack of “clean water” and “safe-water access” as a primary cause of cholera. The intervention in the DRC, which reached 230,000 people with chlorinated water, is a direct action towards this target.
- Target 6.2: “By 2030, achieve access to adequate and equitable sanitation and hygiene for all…” The article points to “inadequate sanitation” as a key driver and mentions the provision of “sanitation facilities” and the promotion of “hygiene measures” as critical interventions.
-
Under SDG 1 (No Poverty):
- Target 1.5: “By 2030, build the resilience of the poor and those in vulnerable situations and reduce their exposure and vulnerability to climate-related extreme events and other economic, social and environmental shocks and disasters.” The article notes that “climate shocks” and “extreme weather events” are compounding factors in cholera outbreaks, which affect vulnerable populations in disaster-hit areas. The anticipatory financing mechanism is a direct example of building resilience to health shocks.
-
Under SDG 17 (Partnerships for the Goals):
- Target 17.2: “Developed countries to implement fully their official development assistance commitments…” The article directly addresses this by discussing the role of the U.S. as the “largest humanitarian donor” and the negative consequences of its “aid freeze,” which led to a decline in “U.S. WASH disbursements.”
-
Under SDG 3 (Good Health and Well-being):
-
Are there any indicators mentioned or implied in the article that can be used to measure progress towards the identified targets?
Yes, the article provides several quantitative and qualitative indicators that can be used to measure progress.
-
For Target 3.3 (End epidemics of water-borne diseases):
- Number of cholera cases: The article reports 462,890 cases from January to August 2025.
- Number of deaths from cholera: It reports 5,869 deaths in the same period.
- Mortality/Fatality Rate: The article notes a “rise in fatalities—up 118 percent” compared to 2024. It also cites the successful intervention in the DRC, which achieved a “case fatality rate of just 0.27 percent,” well below the 1% global benchmark.
- Basic Reproduction Number (R₀): The scientific study cited estimates a median R₀ of 2.0, a direct measure of the disease’s transmissibility.
-
For Target 3.d (Strengthen capacity for early warning and risk management):
- Functionality of surveillance and response systems: The success of the “anticipatory action framework” in the DRC, which linked surveillance to pre-authorized financing, serves as a qualitative indicator of strong capacity.
- Funding for rapid response: The article mentions the release of $750,000 from CERF as an indicator of a functional financing mechanism for health emergencies.
-
For Targets 6.1 and 6.2 (Access to clean water and sanitation):
- Population reached with safe water and sanitation services: The intervention in the DRC reached “more than 230,000 people with chlorinated water, sanitation facilities.” This is a direct indicator of progress.
- Investment in WASH programs: The article implies this indicator by highlighting the negative correlation between the decline in “U.S. WASH disbursements” and the surge in cholera mortality.
-
For Target 17.2 (Official development assistance):
- Humanitarian aid disbursements: The article uses the “U.S. funding freeze” and the subsequent decline in aid for WASH as a clear, albeit negative, indicator related to donor commitments.
-
For Target 3.3 (End epidemics of water-borne diseases):
-
Create a table with three columns titled ‘SDGs, Targets and Indicators” to present the findings from analyzing the article.
SDGs Targets Indicators Mentioned or Implied in the Article SDG 3: Good Health and Well-being 3.3: End epidemics of water-borne and other communicable diseases. 3.d: Strengthen capacity for early warning and management of health risks.
– Number of cholera cases (462,890).
– Number of deaths from cholera (5,869).
– Case Fatality Rate (0.27% in DRC vs. 1% benchmark).
– Basic Reproduction Number (R₀ of 2.0).
– Existence of anticipatory action frameworks.
– Amount of pre-authorized emergency financing ($750,000 from CERF).SDG 6: Clean Water and Sanitation 6.1: Achieve universal access to safe drinking water. 6.2: Achieve universal access to adequate sanitation and hygiene.
– Number of people provided with chlorinated water (230,000 in DRC).
– Number of new sanitation facilities established (implied in DRC intervention).
– Level of funding for WASH programs (e.g., decline in U.S. disbursements).SDG 1: No Poverty 1.5: Build the resilience of the poor and reduce vulnerability to shocks and disasters. – Implementation of programs to mitigate health shocks in disaster-hit areas (e.g., anticipatory action framework).
– Impact of climate shocks and extreme weather events on disease outbreaks.SDG 17: Partnerships for the Goals 17.2: Developed countries to implement official development assistance commitments. – Level of humanitarian aid from major donors (e.g., U.S. aid freeze).
– Collaboration between international agencies (OCHA, WHO, UNICEF) and national governments.
Source: globalbiodefense.com

What is Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
0
Wow
0












